Metabolic Mind or Metabolic Psychiatry
What is Metabolic Psychiatry?
Metabolic psychiatry is an emerging medical subspecialty that focuses on the profound connection between metabolic health and brain function. It operates on the principle that many mental health disorders—such as depression, bipolar disorder, and schizophrenia—are not just “chemical imbalances” but are closely tied to physical metabolic issues like:
- Insulin resistance (how your brain and body process glucose for energy)
- Mitochondrial dysfunction (the cellular powerhouses failing to produce enough energy for the brain)
- Chronic systemic inflammation
- Oxidative stress
The primary intervention in metabolic psychiatry is often Ketogenic Metabolic Therapy (KMT). When the body transitions into ketosis, the brain shifts from burning glucose to burning ketones. This provides a more stable, efficient fuel source, helps balance neurotransmitter levels (such as GABA and glutamate), and calms overactive neural networks.
Is it Reliable or Pseudoscience?
Metabolic psychiatry is not pseudoscience; it is a legitimate, rapidly growing field of scientific inquiry. However, it is still in its emerging stages.
- The Scientific Foundation: It is rooted in over a century of proven neurology. The ketogenic diet has been used successfully since the 1920s to treat drug-resistant epilepsy because of how it stabilizes brain chemistry.
- Active Clinical Trials: Prestigious institutions like Stanford Medicine have led pilot trials demonstrating that a ketogenic diet can significantly improve both metabolic biomarkers (weight, blood sugar, insulin levels) and psychiatric symptoms in patients with bipolar disorder and schizophrenia.
- Current Standing: While the biological mechanisms make perfect sense and early clinical trials are incredibly promising, the field is still developing long-term, large-scale, randomized controlled trials. It is respected by researchers, but is not yet the standard first-line treatment in mainstream clinics.
Can You Rely on It to Stop Your Medication?
CRITICAL SAFETY WARNING:
Never, under any circumstances, stop or adjust your psychiatric medications on your own to start a metabolic diet.
While the ultimate goal for some patients under metabolic care is to reduce or eventually eliminate their medication, doing this without expert supervision is highly dangerous. Here is why:
- Severe Withdrawal and Relapse: Abruptly stopping psychiatric medications (like antipsychotics, mood stabilizers, or antidepressants) can cause severe physical withdrawal, severe rebound symptoms, and acute psychiatric crises (like psychosis or deep depression).
- Keto Changes How Your Meds Work: Transitioning to a high-fat ketogenic diet changes how your liver and kidneys process drugs. It can rapidly alter the absorption and concentration of psychiatric medications in your bloodstream. This can make your current doses suddenly feel toxic (too strong) or completely ineffective.
- Medication Management is Essential: If you choose to adopt metabolic rules (like a medically formulated ketogenic diet), you must work closely with a prescribing physician. A specialist will monitor your blood work, track your ketone levels, and carefully, slowly taper your medications only after your brain has stabilized on the diet.
# Summary: Change Your Diet, Change Your Mind by Dr. Georgia Ede
Core Thesis
Dr. Georgia Ede, a Harvard-trained psychiatrist specializing in metabolic psychiatry, builds her book on one central premise: brain chemistry is fundamentally shaped by food, and dietary intervention can be a primary, not merely adjunctive, treatment for mental illness. She argues that standard psychiatric practice has overlooked the biological origins of neurotransmitters—which are synthesized from nutrients—and that nutritional strategies, particularly ketogenic and low-carbohydrate approaches, can often outperform medication in restoring psychiatric stability.
Structure and Key Arguments
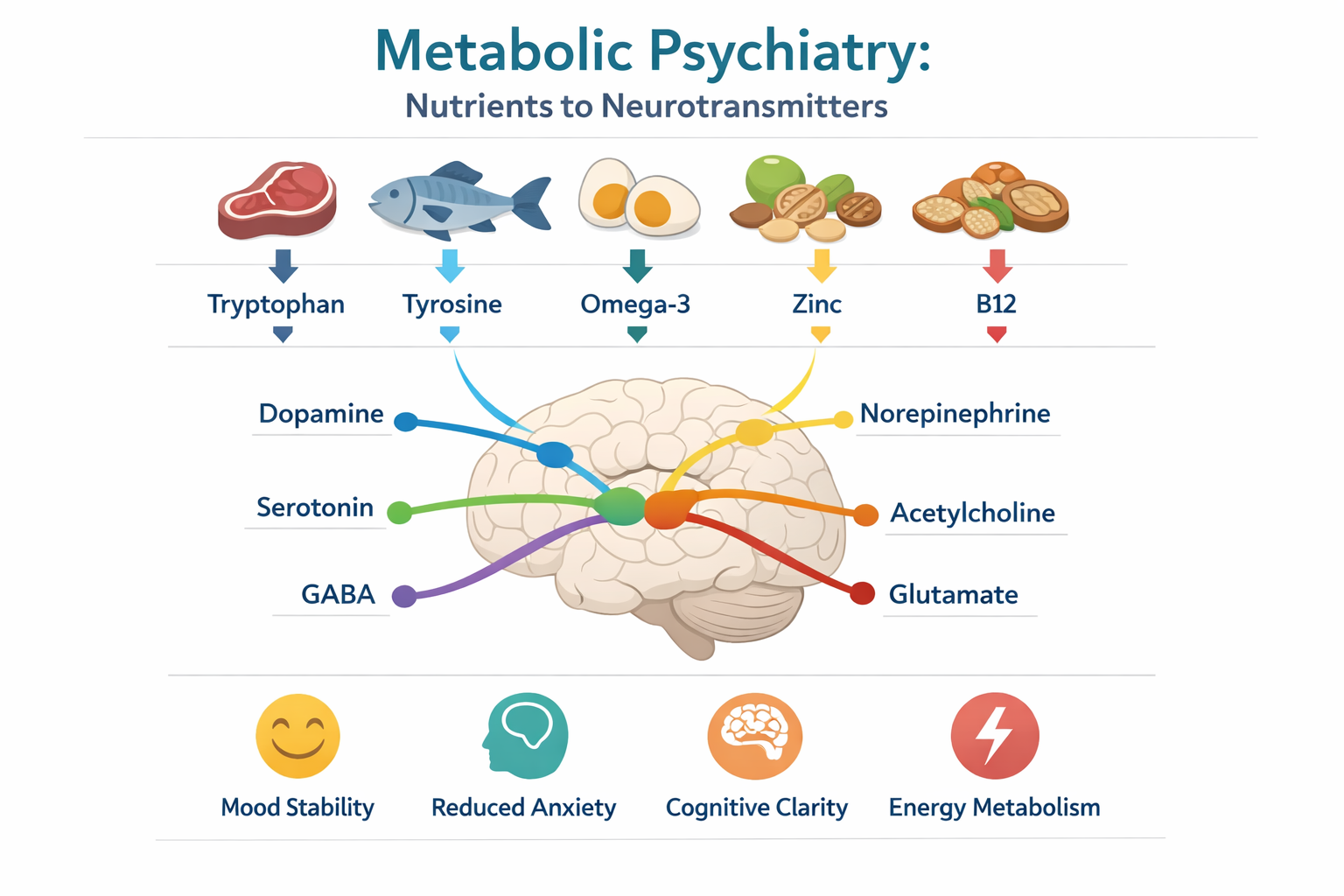
1. The Biochemical Foundation Ede establishes that neurotransmitters (serotonin, dopamine, GABA, acetylcholine) are derived from dietary amino acids, vitamins, minerals, and fatty acids. She emphasizes meat as essential for mental health due to its bioavailability of complete protein, iron, zinc, B12, and long-chain omega-3 fatty acids—nutrients critical for neurotransmitter synthesis and myelination. 2. The Problem with Modern Dietary Guidelines. She critiques conventional “brain-healthy diet” advice (Whole grains, low-fat, Mediterranean) as often counterproductive for metabolically vulnerable individuals. She identifies plant-based diets and high-carbohydrate patterns as potentially contributing to:
- Blood glucose dysregulation
- Chronic inflammation
- Essential nutrient deficiencies (particularly B12, iron, zinc, choline)
- Gut dysbiosis that affects the gut-brain axis
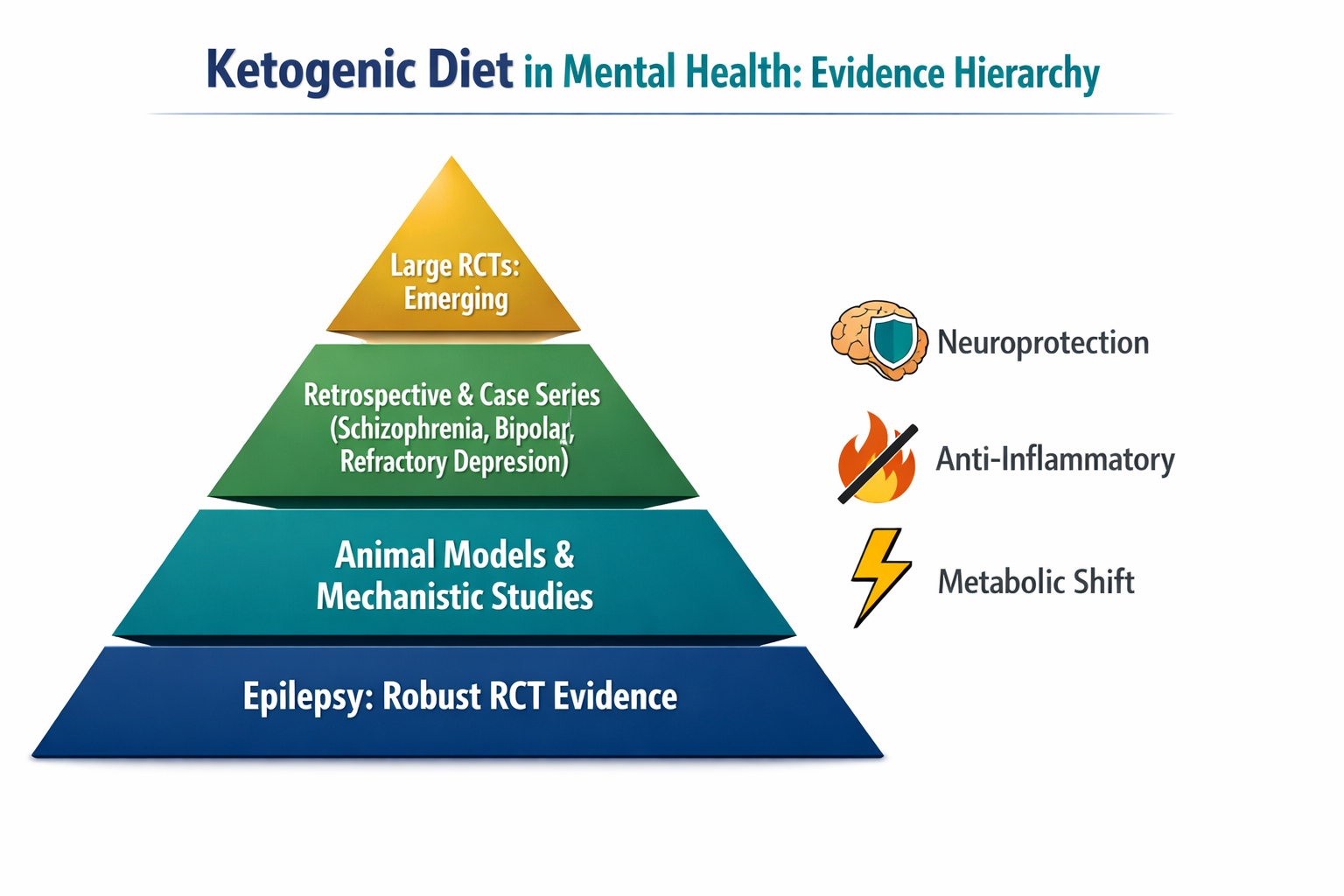
3. The Case for Ketogenic and Low-Carbohydrate Therapy Drawing from both clinical practice and emerging literature, Ede positions the ketogenic diet as:
- Neuroprotective and anti-inflammatory
- Stabilizing for mood, anxiety, and cognition
- Capable of inducing metabolic shifts that reduce oxidative stress in the brain
She extends the ketogenic evidence base beyond its established role in epilepsy into schizophrenia, bipolar disorder, and treatment-refractory depression. 4. Practical Application The book concludes with a prescriptive framework—a “powerful plan” for dietary change designed to improve mood, overcome anxiety, and protect memory over the lifespan.
What the Evidence Actually Shows
From a clinical psychiatry standpoint, it is important to separate the robust from the speculative:
| Claim Domain | Evidence Quality | Clinical Relevance |
|---|---|---|
| Nutrient deficiency → psychiatric symptoms | Well-established | Iron, B12, folate, zinc deficiencies are DSM-5 recognized contributors to cognitive and mood disorders |
| Ketogenic diet in epilepsy | Strong (class I evidence) | Neuroprotective mechanism via mitochondrial biogenesis and stabilization |
| Ketogenic diet in schizophrenia/bipolar | Emerging, retrospective, case-series level | Physiologically plausible (insulin signaling, inflammation, NMDA modulation) but not yet supported by large RCTs |
| Meat as essential vs. plant-based as harmful for mental health | Contested | While bioavailability is higher in animal sources, well-planned omnivorous or supplemented plant-based diets can also achieve nutritional adequacy |
Critical Assessment
Strengths:
- Ede is a credible voice (Harvard psychiatry training, clinical practice in nutritional psychiatry)
- She correctly identifies the metabolic underpinnings of brain disorders as an under-addressed etiological pathway
- The ketogenic approach for refractory mental illness is gaining traction in academic metabolic psychiatry
- The book challenges complacency around dietary counseling in psychiatric practice
Limitations and Caveats:
- Some arguments extrapolate from epilepsy and animal models to mood and psychotic disorders more decisively than current RCT evidence supports
- The anti-plant stance (or strong pro-meat essentialism) may not be necessary; the critical variable may be nutrient density and metabolic control, not the exclusion of plant foods per se
- “Treatment-refractory” populations in published ketogenic psychiatric studies are small and often lack controls
Bottom Line
Change Your Diet, Change Your Mind is a provocative, clinically relevant contribution that forces psychiatrists to take nutrition seriously. It makes the strongest case for metabolic psychiatry as a legitimate subspecialty direction. For an experienced psychiatrist running a daily clinic, the value is not in replacing antipsychotics or mood stabilizers with steak, but in recognizing that:
- Many patients have undiagnosed nutritional deficiencies masquerading as psychiatric syndromes
- Ketogenic therapy may have a role in refractory cases where standard pharmacotherapy fails
- Dietary counseling should be the standard of care, not alternative medicine
The book is worth reading critically, not as dogma, but as a scientific provocation that demands larger, well-controlled trials.